By-pass aorto-coronarian

Cardiac catheterization (Angiogram);
Electrocardiography;
Echocardiography;
Chest x ray; and
Lab tests.
By-pass-ul aorto-coronarian (CABG), din momentul introducerii sale, în perioada anilor '60 s-a dovedit a fi optiunea terapeuticã majorã în tratamentul bolii cardiace ischemice (BCI). Varianta sa "clasicã" cu circulatie extracorporealã (CEC) este o metodã cu rezultate excelente la distantã în special atunci când sunt folosite grefoane arteriale de tipul arterei mamare interne. Totodata, riscurile inerente ale unei interventii chirurgicale complexe, cu mortalitate si morbiditate semnificative, au determinat aparitia si a altor variante tehnice chirurgicale, de tipul CABG pe cord bãtând (OPCABG). S-a dovedit ca, CABG fãrã CEC reduce incidenta efectelor secundare ale chirurgiei clasice , cu pretul aparent al unei revascularizãri incomplete.
Folosirea exclusivã a grefoanelor arteriale are rezultate excelente la distantã, dar expererienta internationalã este limitata la putine centre care o practicã constant pe scara largã.
Folosirea exclusivã a grefoanelor arteriale are rezultate excelente la distantã, dar expererienta internationalã este limitata la putine centre care o practicã constant pe scara largã.

Coronary Artery Bypass Graft Surgery
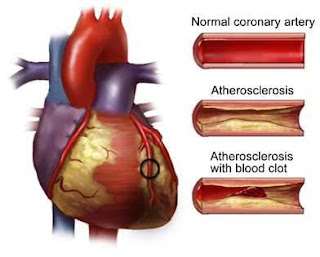
Coronary artery disease, or CAD, is an accumulation of plaque inside one or more coronary arteries that can cause a reduction in blood flow to the heart muscle.
Coronary artery bypass graft surgery, or CABG, is a procedure that improves blood flow to the heart muscle by rerouting blood around the blocked or narrowed portion of a coronary artery.
To reroute blood around a blocked section of a coronary artery, surgeons use a piece of an artery or vein from another part of a person's body, called a bypass graft.
Coronary artery bypass graft surgery, also referred to as bypass surgery and CABG, is the most frequently performed cardiac surgery in the United States.
Bypass surgery is done to restore blood flow to the heart by bypassing arteries narrowed or blocked by atherosclerosis, a process caused by the buildup of fats and cells called plaque. Bypass surgery restores an adequate supply of oxygenated blood to the heart, thus allowing it to work more effectively and efficiently.
This operation is usually performed after drug therapies have failed to improve blood flow and when stenting procedures are not indicated.
PRE-TREATMENT GUIDELINES
Preparation for coronary artery bypass surgery consists of preoperative testing that may include:Cardiac catheterization (Angiogram);
Electrocardiography;
Echocardiography;
Chest x ray; and
Lab tests.
Preparation for heart surgery begins with the shaving and disinfecting of the chest. A narrow, soft tube called an intravenous catheter, or IV, will be placed in one or both of the patient's arms to provide fluids and medication during and after surgery. Another catheter will be placed in the side of the patient's neck. The operation is performed with the patient asleep on a breathing machine.
During the bypass operation, surgeons take a blood vessel from another part of the patient's body and construct a detour around the blocked portion of the coronary artery. One vein that is commonly used to create this detour a greater saphenous vein from the leg. Often, arteries in the chest, such as the left internal mammary artery, or LIMA, are used for grafts. Another vessel used for grafts in coronary artery bypass surgery is the radial artery from the wrist and the forearm, which feeds blood to the hand. Typically, the these vessels are removed by endoscopic vein harvesting through very small incisions.
Almost all coronary bypass surgeries use a heart-lung machine, which enables a surgeon to stop the heart from beating while he or she sews tiny arteries and veins together to form grafts. The heart-lung machine performs the pumping and oxygenation functions of the heart. When the grafts have been completed, the heart is stimulated to begin pumping blood again and the heart-lung machine is removed. Alternatively, the operation can be performed without the heart lung machine. During this "beating heart" procedure, the surgeon is able to see bypasses using small devices that stabilize the movement of the area of the heart being worked on.
Some surgeons now also perform minimally invasive coronary artery bypass (MIDCAB) through small incisions between the ribs. The same techniques are used as in beating-heart surgery, but instead of performing a full sternotomy, or opening the patient's chest by cutting through and separating the breastbone, surgeons make small incisions-or keyholes-between the ribs to access the heart.
Coronary bypass surgery usually takes 2 to 5 hours. After the surgery is completed, the patient typically stays overnight in the intensive care unit of the hospital. The patient is then moved to the cardiac care discharge unit for about 3 to 7 days. Typically, patients are able to walk out of the ICU on their own to the discharge unit.
POST-TREATMENT GUIDELINES
To reduce the chances of developing more disease in the future, the physician will advise the patient certainly to stop smoking and reduce intake of fat and cholesterol. The physician will also recommend that the patient walk or do another form of physical activity to help regain lost strength.
Patients can typically resume driving and other normal activities of daily life by 2 to 4 weeks after surgery. Sexual activity may be resumed in 3 to 4 weeks after surgery.
People with jobs requiring limited physical exertion can typically return to work in 4 to 6 weeks; those with more physically demanding jobs may have to wait longer.
POSSIBLE COMPLICATIONS
There is a small risk of complications from this procedure that includes (but is not limited to):
- Infection;
- Bleeding;
- Heart Failure;
- Breathing problems;
- Blood clots; and
- Stroke or brain damage.
In general, the risk of these complications occuring is less than 5 percent. There is also typically a 2 percent risk of dying from a scheduled coronary artery bypass graft surgery. The risk may increase to 8 percent or higher if other risks are present or it is an emergency procedure.

{kind=link}
Niciun comentariu:
Trimiteți un comentariu
Comentariul Dvs. va fi trimis spre aprobare